Metatarsus Adductus: Diagnosis, Therapy, and Medical Research
Metatarsus Adductus is the most common deformity in newborns.
A metatarsus is a group of bones in the middle section of the foot.
Each foot has five metatarsal bones, each connected to the phalanges of the toes.
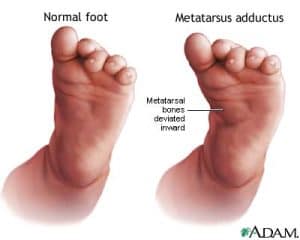
“MA” refers to a condition where the metatarsal bones are turned toward the middle of the body.
This causes a visible deformity, and both feet are often affected.
It is a common congenital condition in infants that is thought to be caused by intra-uterine positioning that leads to abnormal adduction of the forefoot at the tarsometatarsal joint.
May be “flexible” (the foot can be straightened to a degree by hand) or “non-flexible” (the foot cannot be straightened by hand).
Occurs in about 1 newborn of every 12 live births.
Babies with “MA” are at an increased risk for developmental dysplasia of the hip.
In metatarsus adductus, the front part of a child’s foot turns inward.
There is no known cause of “MA”. Metatarsus adductus is a very common foot condition in newborns.
Most of the mild cases of MA resolve without treatment. (Approximately 85%)
However, in up to 14% of affected children, the deformity persists to adulthood.
Many pediatricians regard this deformity as a cosmetic issue of minor functional significance.
However, it is well documented that unresolved “MA” may require further treatment.
Epidemiology
This malformation occurs in approximately 1 in 12 births and has an equal frequency in males and females.
Metatarsus adductus is bilateral in approximately 60% of cases.
There is an increased incidence in late pregnancy, first pregnancies, twin pregnancies, and oligohydramnios.
Associated conditions include DDH (15-20%) and torticollis.
Although most mild cases of “MA” resolve by the time of skeletal maturity, the persistence of the deformity has been associated with the development of hallux valgus (HV).
The incidence of MA in patients with HV was reported to be 21.6% to 29.5%.
Causes
It’s thought to be caused by the infant’s position inside the womb.
Risks may include that the baby’s bottom was pointed down in the womb (breech position) or the mother had a condition called oligohydramnios, in which she did not produce enough amniotic fluid.
There may also be a family history of the condition.
Diagnose of Metatarsus Adductus
This deformity can be diagnosed through a physical exam. Telltale signs of this condition include the high arch and a visibly curved and separated big toe.
During the examination, the doctor will obtain a complete birth history of the child and ask if other family members were known to have metatarsus adductus.
Diagnostic procedures are not usually necessary to evaluate metatarsus adductus.
However, X-rays (a diagnostic test that uses invisible electromagnetic energy beams to produce images of internal tissues, bones, and organs onto film) of the feet are often done in the case of nonflexible metatarsus adductus.
An infant with metatarsus adductus has a high arch and the big toe has a wide separation from the second toe and deviates inward.
Flexible metatarsus adductus is diagnosed if the heel and forefoot can be aligned with each other with gentle pressure on the forefoot while holding the heel steady.
This technique is known as passive manipulation.
If the forefoot is more difficult to align with the heel, it is considered a nonflexible, or stiff foot.

Metatarsus Adductus Treatment For Infants
The best time to treat Metatarsus Adductus is under the age of 9 months only.
The main reason is that the infant’s joints are more flexible and can be treated effectively.
Until 2018 the most common method in the last 200 years was serial casting.
The game completely changed in 2018 when a brilliant doctor from Israel- D.R Izak Daizade invented the special brace that solves the MTA issues for newborns until 9 months.
Solution number 1- Complicated Surgery
Option 1 to treat metatarsus adductus is complicated surgery among infants, children, and adults.
Usually, the surgery can not guarantee 100% success.
Solution number 2- Serial casting
Option 2 is by Serial casting unfortunately is still the most popular method today worldwide to treat infants until 9 months.
The procedure is to use serial casting for almost 2 months from the foot to the hips.
Solution number 3- UNFO Brace

The best solution for metatarsus adductus today is by wearing the UNFO shoes/brace.
The UNFO brace is an approved FDA & CE product and it is the most advanced treatment method and the easiest one for babies until 9 months worldwide.
The treatment is straightforward, we use the shoes for 6 weeks and we get 95-98% straight foot after 2 to 3 weeks.
We wear another 3 weeks to remain the results we achieved during the first 3 weeks.
for more information please visit our guide page for parents and professionals.
You also can check our success stories we treated successfully thousands of children that suffered from MTA around the globe.
Treatment of Metatarsus Adductus
Specific treatment for this foot deformity will be determined by your child’s doctor based on your child’s age, overall health, and medical history, the extent of the condition your child’s tolerance for specific medications, procedures, or therapies, expectations for the course of the condition and your opinion or preference.
In light of reports that 10–14% of metatarsus adductus cases persist to adulthood and some require surgical intervention, a more proactive approach is advocated by some authors for rigid, severe deformities The goal of treatment is to straighten the position of the forefoot and heel.
Treatment options vary widely from watchful follow-up, passive stretching, bracing, serial casting, and, rarely, surgical correction Studies have shown that metatarsus adductus may resolve spontaneously (without treatment) in the majority of affected children, only in the easy cases f MTA.
The Deformity doesn’t resolve itself in most of the advanced cases of MTA, it doesn’t resolve itself in the hard cases of the MTA, if the infant is not treated in the window time, which is under the age of 9 months, it can be too late later.
When to use the UNFO Brace?
IT is very hard to treat MA with the UNFO Brace or even with serial casting when the child stands to his tfeet and starts walking.
This deformity gets further complicated by the notion that early intervention, before 8 to 9 months of age, when spontaneous improvement is more likely, carries a better chance for deformity improvement.
When more severe, less flexible MTA is present, bracing or serial casting is often recommended with reported long-term success rates of approximately 95%.
A doctor or nurse may instruct you on how to perform passive manipulation exercises on your child’s feet during diaper changes.
A change in sleeping positions may also be recommended. Suggestions may include side-lying positioning.

Does stretching work?
In rare instances, the foot does not respond to the stretching program, long leg casts may be applied.
Casts are used to help stretch the soft tissues of the forefoot.
The plaster casts are changed every 1 to 2 weeks by your child’s pediatric orthopedist.
If the foot responds to casting, straight-cast shoes may be prescribed to help hold the forefoot in place.
Straight last shoes are made without a curve in the bottom of the shoe.
For those infants with very rigid or severe metatarsus adductus, surgery may be required to release the forefoot joints.
Following surgery, casts are applied to hold the forefoot in place as it heals.
There are several outcome studies of this most common deformity in newborns, with most patients presenting with benign and self-limiting metatarsus adductus.
However, there are numerous reports of unresolved metatarsus adductus treated surgically.
Therefore, it would seem that before surgical intervention, most children with resistant metatarsus adductus should be actively treated with casts or orthoses, potentially decreasing the need for subsequent surgical procedures.
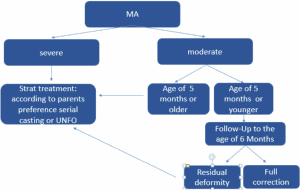
A recent meta-analysis emphasized the importance of an accurate initial determination of the severity of metatarsus adductus to be able to decide the appropriate treatment strategy.
For mild, flexible metatarsus adductus, observation is suggested.
More rigid metatarsus adductus should be treated with casting/bracing.
This study also stresses the lack of perspective, randomized clinical trials

Medical Research
Avi Panski, Naum Simanovski, Vladimir Goldman, Ron Lamdan Pediatric Orthopedics Unit,
Hadassah medical center, Jerusalem


Metatrasus Adductus (MA), what do we know?
The most common foot deformity in newborns: 1-2/1000 births
Treatment of Metatasus Adductus
Materials and methods
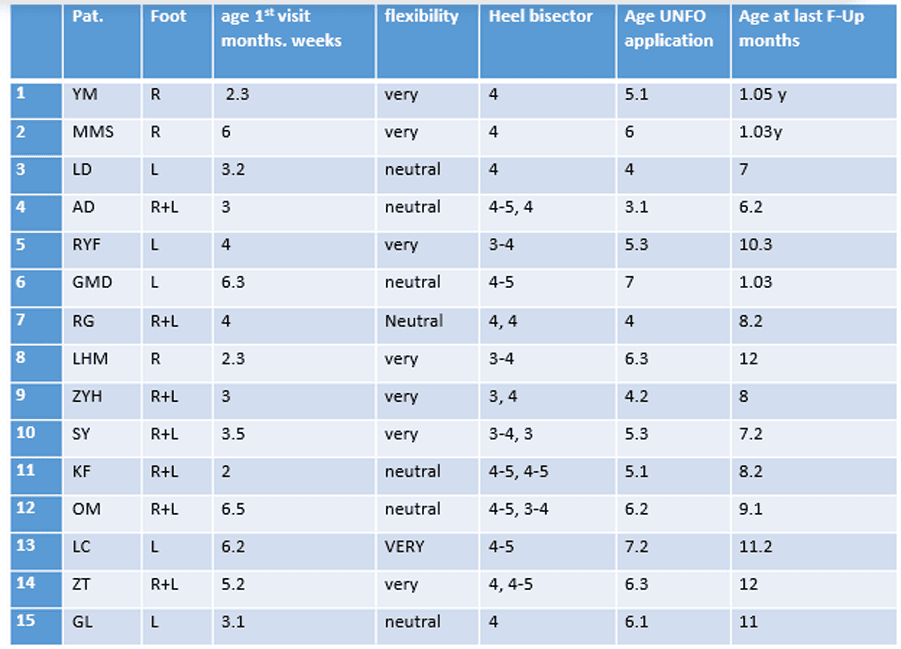
• Retrospective study of our first 15 consecutive patients treated with UNFO (June 2014 – November 2015)
• Follow up of 2 months minimum after cessation of treatment
• Treatment protocol:
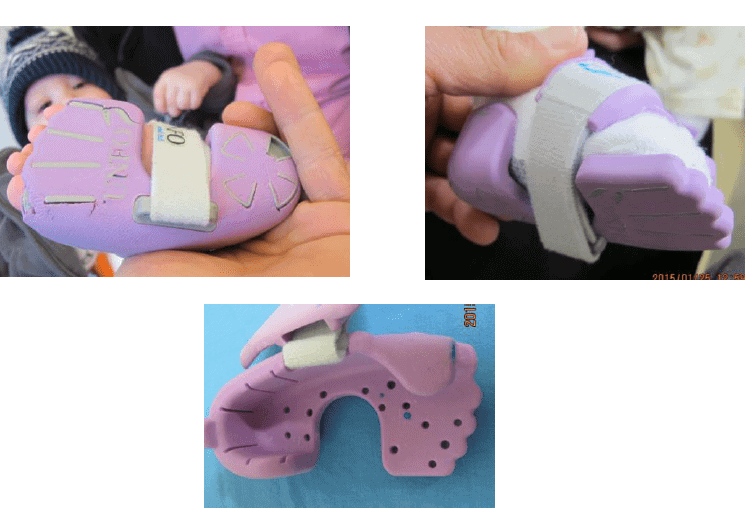
What is UNFO
Universal Foot Orthotics
2 sizes
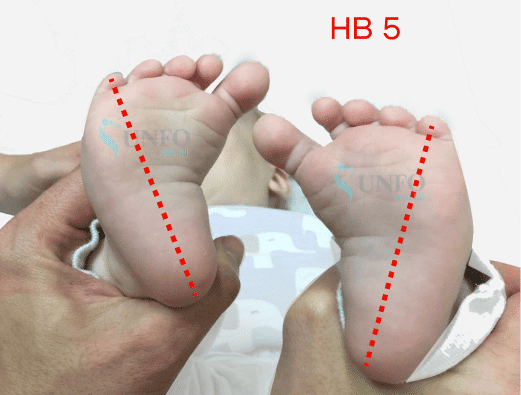
3 point pressure
Heel held firmly
Point of pressure against the 1st metatarsal head
Strap for increasing pressure gradually over base of 5th metatarsus
UNFO treatment protocol
• UNFO was first applied for 23 hours a day
•Weaning gradually when full correction was achieved
•3-4 weeks 18 hours
• 3-4 weeks 12 hours night time
• Stop UNFO
• (if the parents wish, continue night time bracing as long as it fits)
• Follow-up 3 week
• Follow-up when walking
• Follow-up at the age of 1.5 and 2 years
Patients details